What is the bicep?
The biceps muscle is located on the front of the arm and extends from the shoulder passed the elbow to the radius. At the shoulder, the bicep tendon connects with two tendons. The long head of the bicep attaches in the shoulder at the labrum/glenoid while the short head attaches to the coracoid. At the elbow the bicep attaches to the radius.
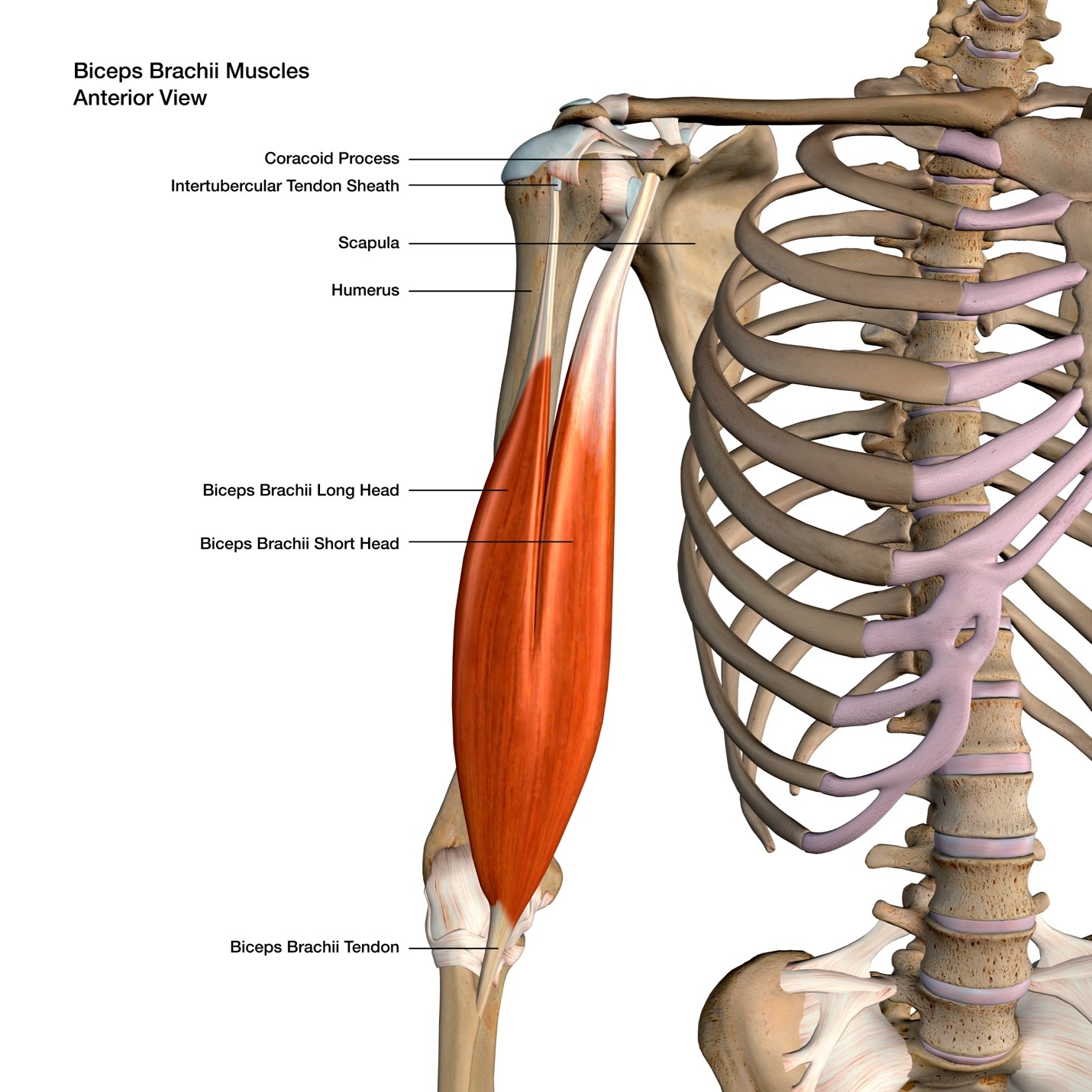
Figure 1 Anterior view of the biceps muscle and tendon. Shown are the two proximal attachments and single distal attachment. Licensed from Adobe stock.
What is the function of the bicep muscle?
The bicep muscle functions to flex the elbow as well as to turn the palm of the hand upwards (supination).
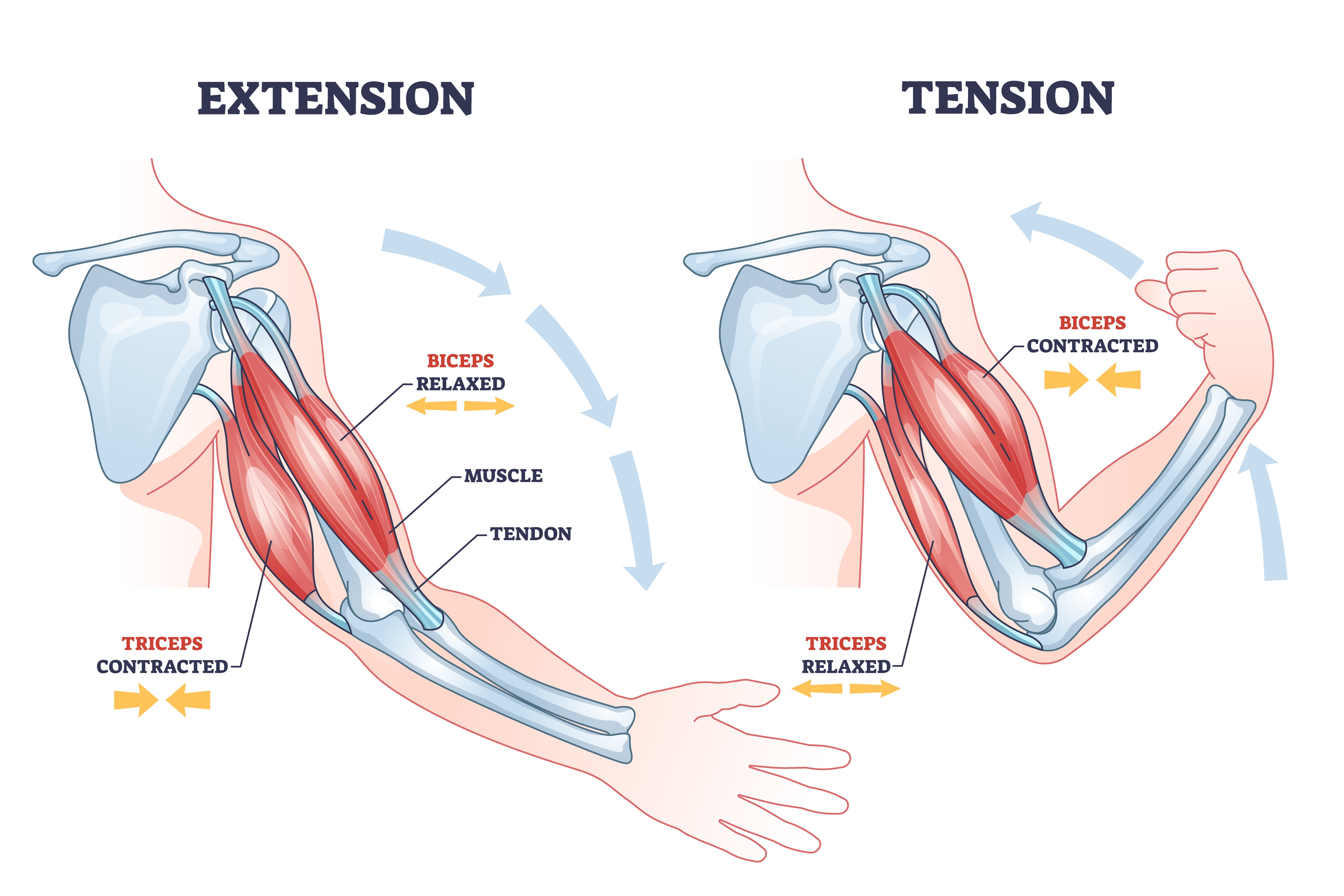
Figure 2 Example of contraction and relaxation of bicep and tricep muscles. Licensed from Adobe stock.
How is the bicep tendon torn?
Complete tears of the bicep tendon occur during a forceful eccentric contraction of the muscle.
Examples include catching a falling object or a shifting of an objects weight while carrying the object resulting a sudden forceful elongation of the muscle.
Partial tearing can also occur in a similar fashion or can also occur with repetitive use.
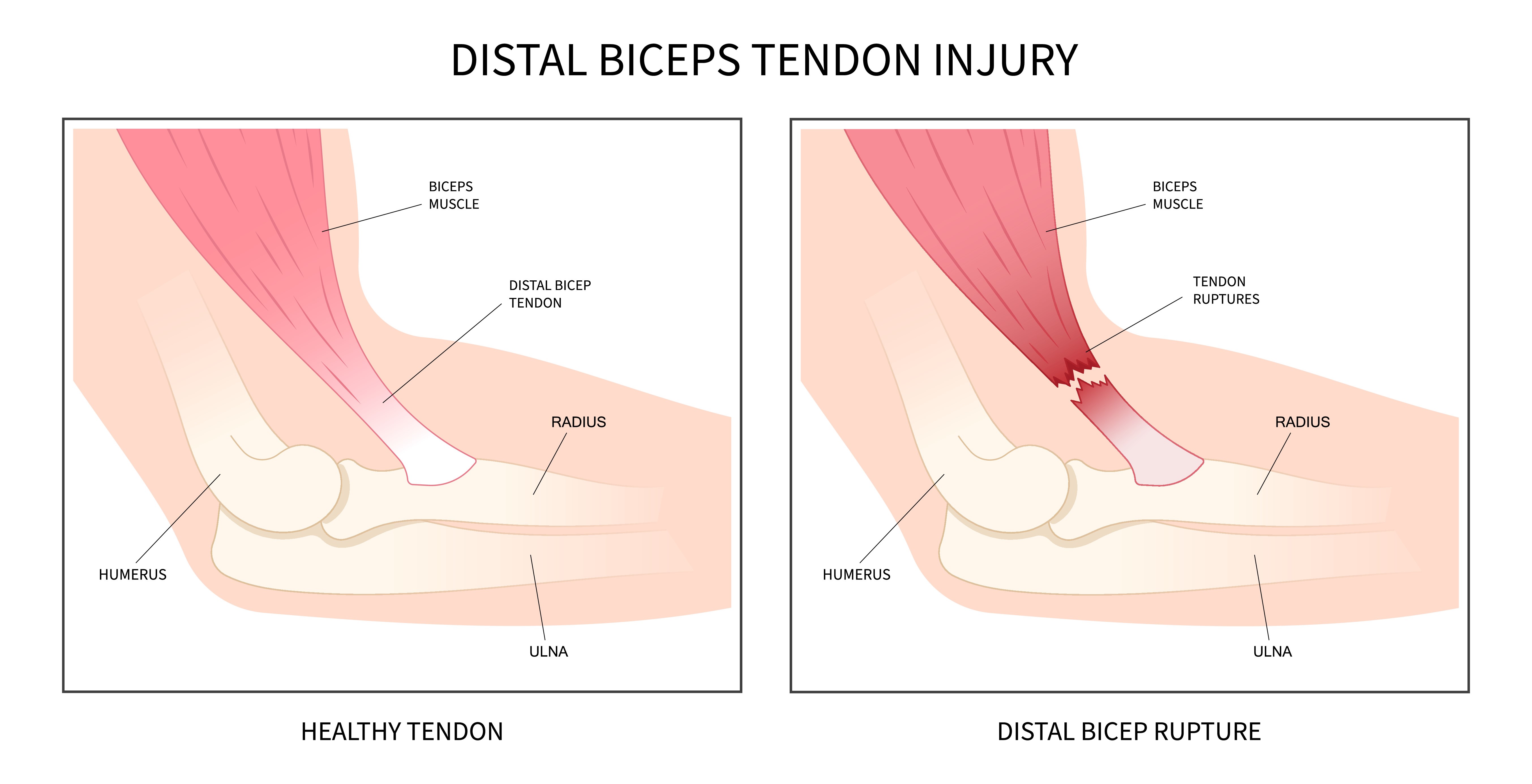
Figure 3 Demonstration of distal biceps rupture. Licensed from Adobe stock.
What are the symptoms of a bicep tendon tear?
With complete tears of the bicep tendon, you may feel a pop in the elbow as the tear occurs.
Following the tear there is often pain, swelling and bruising at the elbow. There may also be a visible deformity of the bicep tendon as the muscle retracts up the arm. For some there may be stiffness in the elbow secondary to pain. There may also be weakness in elbow flexion and forearm supination.
How is a bicep tendon tear diagnosed?
Complete tears are often apparent based on the history of the injury and examination of the patient.
There will often be an obvious deformity to the bicep tendon. A hook test can be performed to examine for the presence of an intact tendon. The test is performed by hooking the examiners finger around the bicep tendon at the elbow. In some cases, an ultrasound or an MRI can be used to determine or confirm the diagnosis.
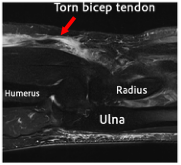
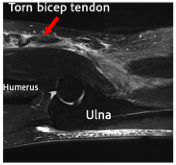
Figure 4 Examples of MRIs of the elbow demonstrating a torn bicep tendon.
What are the treatment options for a bicep tendon tear?
For complete tears of the distal bicep tendon, surgical repair often provides a superior outcome.
For some patients, conservative care may yield a pain free elbow but often with a resulting, weakness in forearm supination and elbow flexion. There would also be a permanent deformity from the torn biceps tendon. For some patients, they may also continue to have cramping pain in the torn biceps. Surgical repair, often leads to full range of motion of the elbow and improved elbow strength when compared to conservative care.
For partial tears, treatment will often depend on percentage of the tendon that is torn, length, of symptoms and other patient specific factors such as occupation and activity level. Often conservative care is initially trialed to include activity modification, NSAIDs, and physical therapy.
Some small studies have also shown promising results from platelet rich plasma injections. For tears that involve 50% or greater of the tendon, or for tears that have not responded to conservative care, surgery is also an option. Surgery typically involves debridement of then tendon with or without detachment and reinsertion of the torn tendon.
How is the biceps repair performed?
A roughly 3-4 - centimeter incision is made on the forearm overlying the biceps insertion. The biceps tendon is then identified and a suture is placed in the biceps tendon. A hole is then drilled in the radius at the biceps insertion site. A small metal button is then passed through this drill hole and used as a pulley to bring the torn bicep tendon back to the insertion. The suture is then tied. In cases of chronic or recurrent ruptures a graft may be needed to add length to the biceps for reinsertion.
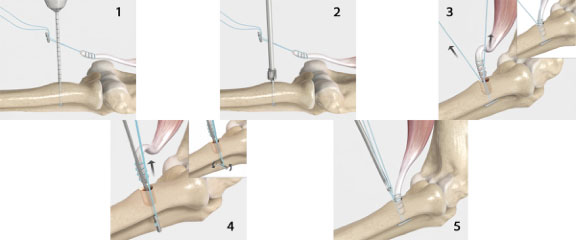
Figure 5 Steps to bicep tendon repair. Credit: Arthrex.com
Timing of distal biceps repair surgery
Repairing the bicep tendon sooner rather than later is preferred. Ideally repair can be performed in the acute setting (less than 3 weeks). Surgery performed in the chronic setting may result in the need for additional dissection, larger incisions, and possible need for grafts for the repair.
Outcomes of distal biceps repair
Outcomes of distal biceps repair are often good to excellent. Most patients are able to return to prior sporting activities. An example of one studies outcome is noted below.
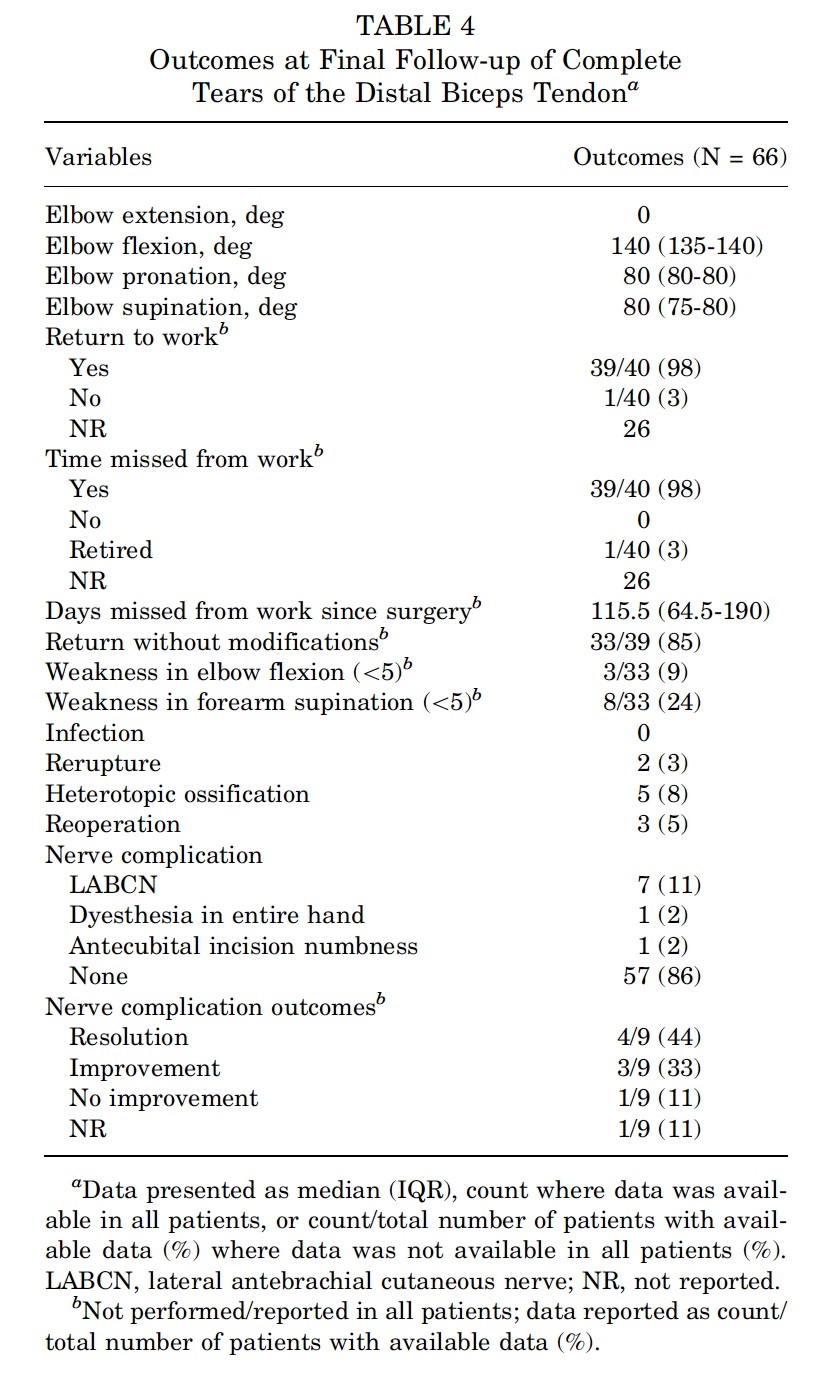
Figure 6 Tagliero AJ, Till SE, Pan X, et al. Long-term Outcomes of Complete Tears of the Distal Biceps Tendon: An Analysis of Surgical Management at a Median Follow-up of 14.7 Years. Orthopaedic Journal of Sports Medicine. 2024;12(10). doi:10.1177/23259671241283787
Return to sport after distal biceps repair
The rate of return to sport after distal biceps repair is high. Many studies report return to sport rates of 85-100%. Return to the same level of sport is lower with some studies showing a ~60% return to same level of sport despite > 90% return to sport rate. The length of time is variable, depending on the sporting activity. Many studies report return timing at ~6-12 months after surgery.
What are the possible complications after distal bicep repair surgery?
Infection
Infection is an uncommon complication after this type of surgery. Rates are typically below 2% for any type of infection with rates of deep infection being less than 1%. Prevention at the time of surgery includes the surgical sterilization of the skin and using the use of antibiotics at the time of surgery. Presentation of infections could include fever, chills, increased pain and swelling at the surgical site, redness, warmth and drainage. Management often includes antibiotics and possibly surgical irrigation and debridement.
Nerve Injury
Major nerve injury is uncommon. Nerve injury that affects the motor component is reported at ~2%.
The majority of these cases resolved with continued observation. In some cases a surgery for nerve repair or tendon transfer was needed. A more common minor nerve injury can affect one of the nerves providing sensation to the forearm. This can result in an area of decreased sensation and can occur in ~10% of cases. This typically resolves with observation.
Re-rupture
Re-rupture is also an uncommon complication. This has also been reported at ~2%. This can occur from a new trauma after the surgery. This may require a repeat surgery for repair.
Vascular Injury
Injury to the brachial artery has been reported but is extremely rare. Injury to this artery requires a vascular repair.
Other reported complications
Other reported complications include elbow stiffness, radius fracture, complex regional pain syndrome and compartment syndrome.
This is not an exhaustive list of all complications. Other complications, although uncommon, can still occur.
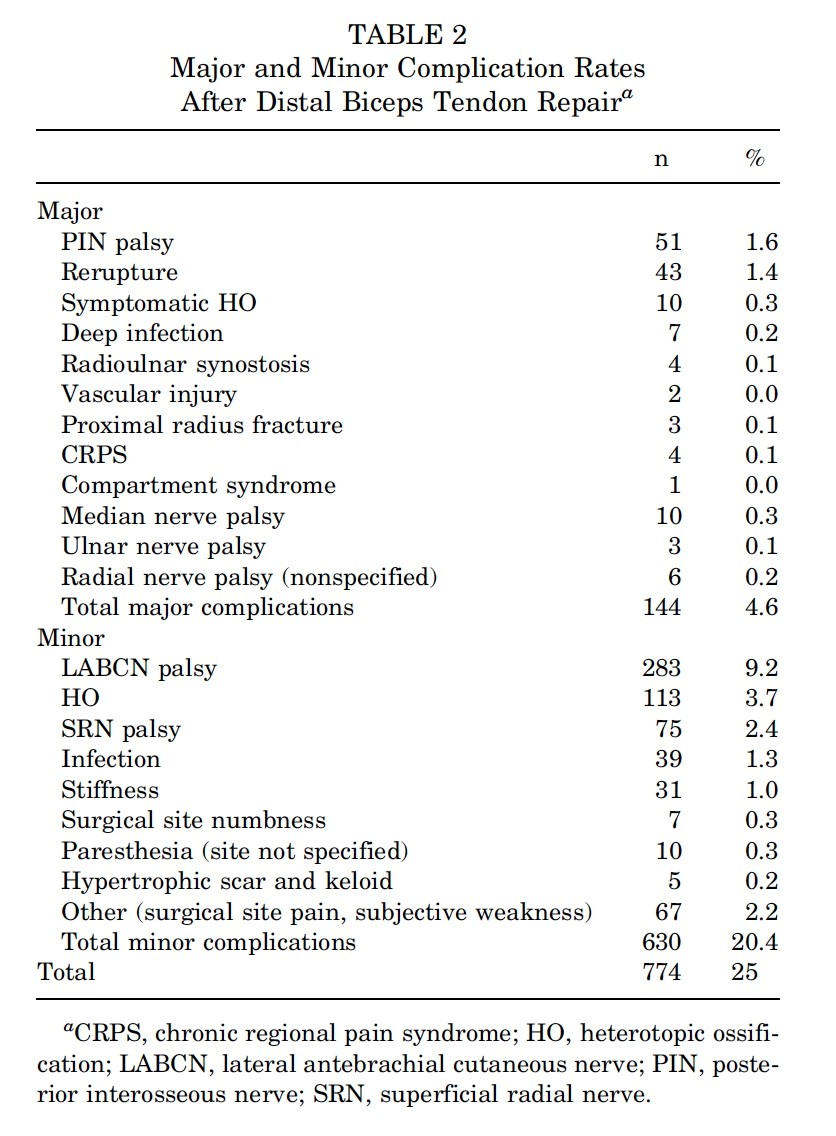
Figure 7 Amarasooriya M, Bain GI, Roper T, Bryant K, Iqbal K, Phadnis J. Complications After Distal Biceps Tendon Repair: A Systematic Review. Am J Sports Med. 2020 Oct;48(12):3103-3111. doi: 10.1177/0363546519899933. Epub 2020 Feb 24. PMID: 32091914.
What will help my pain after surgery?
Medications including narcotic pain medications and anti inflammatories may be prescribed after surgery to help reduce pain. Nerve blocks at the time of surgery have been shown to be affective at reducing pain with low risk of long term deficits.
Do I need to use a brace after my distal bicep repair surgery?
Most patients will not need to be splinted or use a brace after surgery. Patients will often use a sling for comfort but can begin self directed range of motion immediately following surgery. In certain cases, such as chronic or revision surgeries, a brace or splint may also be utilized.
When can I return to work after surgery?
Return to work will largely depend on your specific occupational requirements. Many patients are no longer requiring the use of pain medications during the day by the second to fifth day after surgery. If your work is sedentary, you may be able to return as soon as this time. Work that involves heavy lifting may require longer periods away from work if light duty is not available.
When can I drive after surgery?
There is no definitive test we can do to determine when a patient is safe to return to driving. You should not be taking narcotic or sedating medications prior to driving. You should also not need the use of a sling. No study has been completed demonstrating when it is safe to return to driving after distal bicep repair. In general, a patient should possess the strength and range of motion to utilize the vehicles steering wheel in all situations prior to driving.
Post operative Instructions
- Following your stay in the recovery room and when your vital signs are stable you will be discharged to your escort.
- Remember, it is normal to feel a little dizzy or drowsy for several hours after surgery. This is due to the action the medicine used during surgery.
- If you do not have a post operative appointment scheduled, please call the office as soon as possible to schedule this appointment.
- Take your pain medicine as directed. Begin the pain medicine before you start getting uncomfortable, as the nerve block will wear off. If you wait to take your pain medication until the pain is severe, you will have more difficulty in controlling the pain.
- If you are taking narcotic pain medication you may need a stool softener to prevent constipation. Over-the-counter medication such as Docusate or Milk of Magnesia is recommended.
- Notify the office of any fever, chills, or temperature > 100.5.
- Notify the office of any wound drainage.
Post-Surgery Diet
Resume your diet as tolerated and include vegetables, fruits, and proteins (such as meats, fish, chicken, nuts, and eggs) to promote healing. Also, remember to have adequate fluid intake. It is common after surgery to lack an appetite. This may be the result of anesthesia and the medications. Proper nutrition is needed for healing. During the healing process, the body needs increased amounts of calories and protein. Eat a variety of foods to get all the calories, proteins, vitamins, and minerals you need. If you have been told to follow a specific diet, please follow it.
How should I manage my surgical site and bandages?
You can remove your surgical dressing on the second day after your surgery. Your incision may still have skin glue present. The skin glue can be left in place. You can shower at this time. You do not need to cover the incision unless the wound is irritated by clothing.
What is my activity level after surgery?
You will use a sling for comfort. It is okay to remove the sling as tolerated and move the elbow. You should not be lifting with the elbow. You can also move your wrist and fingers as tolerated.
Can I smoke following surgery?
You should not smoke after surgery as it interferes with healing.
Questions or Concerns
If at anytime you have questions or concerns you can either contact your surgeon’s medical assistant via email or you can call the main office numbers at: (855) 624-3306. You can also use the electronic medical record’s online portal to send questions.
Example rehabilitation protocol:
| Post-OP Week 1-2: | Begin: |
|---|---|
| Goals: | 1. Minimize swelling and pain 2. Full forearm supination and pronation 3. Elbow ROM from 30° of extension to 130° of flexion advancing to 0 ° of extension as tolerated |
| Exercises: | 1. ROM Elbow as above 5-6 times per day 2. AROM Shoulder |
| Weeks 3-6: | Begin: |
|---|---|
| Goals: | 1. Full elbow and forearm ROM by 6 weeks |
| Exercises: | 1. Week 3: ACTIVE Elbow extension to 0°. PASSIVE flexion may be increases to full flexion as tolerated 2. Week 3: ACTIVE Wrist flexion extension, full hand ROM, ACTIVE supination/pronation 3. Week 4: begin Putty for grip strength, pulley ROM exercises 4. Week 5: ACTIVE Elbow extension to full, begin supine scapular stabilizations (no weight), door ABCs or Circles with ball 5. Week 6: PASSIVE Elbow extension to full as needed 6. Week 6: Begin light tubing or 1-kg weights for elbow flexion/extension, forearm rotation and wrist flexion/extension, supine scapular stabilizations 7. Week 6: Begin ball toss/trampoline toss, shoulder theraband strengthening |
| Weeks 7+: | Begin: |
|---|---|
| Goals: | 1. Normalize elbow strength |
| Exercises: | 1. Begin strengthening exercises to wrist, forearm, and possibly shoulder, depending on sport and/or work requirements |
- Amarasooriya M, Bain GI, Roper T, Bryant K, Iqbal K, Phadnis J. Complications After Distal Biceps Tendon Repair: A Systematic Review. American Journal of Sports Medicine. 2020;48(12):3103-3111. doi:10.1177/0363546519899933
- Tagliero AJ, Till SE, Pan X, et al. Long-term Outcomes of Complete Tears of the Distal Biceps Tendon: An Analysis of Surgical Management at a Median Follow-up of 14.7 Years. Orthop J Sports Med. 2024;12(10). doi:10.1177/23259671241283787
- Phelps BM, Birnbrich A, Singer W, Bohle K, George A, Jack RA. Postoperative rehabilitation and return to sport criteria following distal biceps tendon rupture surgery. JSES Int.Elsevier B.V. 2025;9(3):929-933. doi:10.1016/j.jseint.2025.02.013
- Vis J van der, Janssen SJ, Bleys RLAW, Eygendaal D, Bekerom MPJ van den. Distal biceps tendon injection. Clin Shoulder Elb. 2021;24(2):93-97. doi:10.5397/cise.2021.00010
- Kolaczko JG, Knapik DM, McMellen CJ, Mengers SR, Gillespie RJ, Voos JE. Complete Isolated Ruptures of the Distal Biceps Brachii During Athletic Activity: A Systematic Review. Cureus. Published online August 11, 2022. doi:10.7759/cureus.27899
- Alkaduhimi H, Hilgersom NFJ, Eygendaal D, van den Bekerom MPJ, Oh L. The Outcomes of Soft-Tissue Repair for Posterior Shoulder Instability Surgery. Archives of Bone and Joint Surgery. 2022;10(1):45-51. doi:10.22038/ABJS.2021.41491.2121
- Jansen N, Zweers L, Verstuyft L, van Riet R, Caekebeke P. Efficacy of conservative treatment strategies for partial distal biceps tendon ruptures: a case-control study. J Shoulder Elbow Surg. Published online 2025. doi:10.1016/j.jse.2025.04.017
- Clark DS, Moore BP, Somerson JS. Sensory neurapraxia after distal biceps repair is not associated with patient-reported outcomes or satisfaction: a retrospective cohort study. J Shoulder Elbow Surg. 2024;33(12):2695-2701. doi:10.1016/j.jse.2024.05.059
- Dave U, Mosalakanti J, Guduri P, Rumps M, Mulcahey MK. Heterotopic ossification (HO) prophylaxis after distal biceps repair. JSES Reviews, Reports, and Techniques.Elsevier Inc. 2024;4(4):715-719. doi:10.1016/j.xrrt.2024.05.012
- Dauzère F, Laumonerie P, Ollivier I, Antoni M, Clavert P. Anatomy of the biceps brachii osseous footprint: study of 100 radii and literature review. Hand Surg Rehabil. 2023;42(1):24-27. doi:10.1016/j.hansur.2022.11.005
- Fones L, Plusch K, Wiafe BM, Gibbons JL, Beredjiklian PK. Early Postoperative Complications Following Partial Distal Biceps Tendon Surgical Repair. Journal of Hand Surgery. Published online 2025. doi:10.1016/j.jhsa.2025.04.012
- Bajwa A, Simon MJK, Leith JM, Moola FO, Goetz TJ, Lodhia P. Surgical Results of Chronic Distal Biceps Ruptures: A Systematic Review. Orthop J Sports Med.SAGE Publications Ltd. 2022;10(1). doi:10.1177/23259671211065772
- Schmidt GJ, Fischer JP, Crosby NE, Hoyer RW. Clinical Outcomes of Surgical Repair for Partial Distal Biceps Tendon Tears. Journal of Hand Surgery. 2024;49(9):930.e1-930.e8. doi:10.1016/j.jhsa.2022.11.015
- Parikh P, MacDermid JC, Tuli V, Manley M. Distal biceps tendon rupture: Is surgery the best course of treatment? Two case reports. Journal of Hand Therapy. 2021;34(3):463-468. doi:10.1016/j.jht.2020.03.013
- Khaliq M, Giannoudis VP, Palan J, Pandit HG, van Duren BH. Return to driving post upper or lower extremity orthopaedic surgical procedures: a scoping review of current published literature. EFORT Open Rev. 2023;8(12):936-947. doi:10.1530/EOR-23-0117
- Boyle AB, George CM, MacLean SBM. Anatomic factors associated with partial distal biceps tendon tears: a comparative control study. J Shoulder Elbow Surg. 2022;31(6):1224-1230. doi:10.1016/j.jse.2022.01.149
- Yari S, Qawasmi F, Nelson JP, McGrady LM, Grindel SI, Wang M. Biomechanical Comparison of Two Surgical Repair Techniques of the Distal Biceps Tendon. J Hand Surg Glob Online. 2023;5(3):344-348. doi:10.1016/j.jhsg.2023.03.004
- Bergman JW, Silveira A, Chan R, et al. Is Immobilization Necessary for Early Return to Work Following Distal Biceps Repair Using a Cortical Button Technique?: A Randomized Controlled Trial. Journal of Bone and Joint Surgery. 2021;103(19):1763-1771. doi:10.2106/JBJS.20.02047
- Baylor JL, Kloc A, Delma S, Foster BK, Grandizio LC. Impact of Bracing and Therapy Services on Perioperative Costs for Patients Undergoing Distal Biceps Tendon Repair. Journal of Hand Surgery. 2025;50(1):94.e1-94.e8. doi:10.1016/j.jhsa.2023.04.019
- Rutka V, Weppe F, Duprey S, Gras LL. Distal biceps tendon repair via new knotless endobutton fixation: A biomechanical study. Shoulder Elbow. 2021;13(3):321-328. doi:10.1177/1758573219864303
- Caekebeke P, Schenkels E, Bell SN, van Riet R. Distal Biceps Provocation Test. Journal of Hand Surgery. 2021;46(8):710.e1-710.e4. doi:10.1016/j.jhsa.2020.12.012
- Albishi W, Agenor A, Lam JJ, Elmaraghy A. Distal Biceps Tendon Tears: Diagnosis and Treatment Algorithm. JBJS Rev.Journal of Bone and Joint Surgery Inc. 2021;9(7). doi:10.2106/JBJS.RVW.20.00151
- Taylor AL, Bansal A, Shi BY, Best MJ, Huish EG, Srikumaran U. Optimizing Fixation for Distal Biceps Tendon Repairs: A Systematic Review and Meta-regression of Cadaveric Biomechanical Testing. American Journal of Sports Medicine. 2021;49(11):3125-3131. doi:10.1177/0363546520986999
- Caekebeke P, Duerinckx J, van Riet R. Acute complete and partial distal biceps tendon ruptures: what have we learned? A review. EFORT Open Rev. 2021;6(10):956-965. doi:10.1302/2058-5241.6.200145
- Garlapaty AR, Jones M, Baumann J, Gunn C, Cook JL, DeFroda SF. Characterization of distal biceps tendon and triceps tendon injuries in National Football League players from 2009 to 2022. J Orthop. 2025;68:20-26. doi:10.1016/j.jor.2025.01.033
- Dworkin JD, Schmidt CC, Cooke SP, et al. The pathoanatomy of atraumatic partial distal biceps tears: a cadaveric study. JSES Int. 2023;7(3):506-510. doi:10.1016/j.jseint.2023.01.004
- Vishwanathan K, Soni K. Distal biceps rupture: Evaluation and management. J Clin Orthop Trauma. 2021;19:132-138. doi:10.1016/j.jcot.2021.05.012
- Qazi S, Regal S, Greco V, et al. Biomechanical analysis of single-incision anatomic repair technique for distal biceps tendon rupture using tunneling device. Shoulder Elbow. 2023;15(2):195-206. doi:10.1177/17585732211034818
- Besmens IS, Guidi M, Schiller A, Jann D, Giovanoli P, Calcagni M. Management of posterior interosseous nerve (PIN) palsies after distal biceps tendon repair using a single incision technique- a conclusive approach to diagnostics and therapy. J Plast Surg Hand Surg. 2021;55(4):226-231. doi:10.1080/2000656X.2020.1858841
- Garvin PM, Wellington IJ, Connors JP, et al. Bicortical suspensory button fixation yields greater ultimate load to failure over unicortical all-suture anchor fixation in distal biceps brachii tendon repair. J Shoulder Elbow Surg. 2022;31(11):2347-2357. doi:10.1016/j.jse.2022.04.021
- Forlenza EM, Lavoie-Gagne O, Parvaresh KC, Berlinberg EJ, Agarwalla A, Forsythe B. Two Intramedullary and 1 Extramedullary Cortical Button, With or Without Interference Screw, Show Biomechanical Properties Superior to Native Tendon in Repair of the Distal Biceps Tendon: A Systematic Review and Network Meta-analysis of Biomechanical Performance. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2023;39(2):390-401. doi:10.1016/j.arthro.2022.08.037
- Ernstbrunner L, Almond M, Rupasinghe HS, et al. Biomechanical Comparison of Distal Biceps Tendon Repair Techniques: Extracortical Single-Button Inlay Fixation Versus Intracortical Double-Button Onlay Anatomic Footprint Fixation. American Journal of Sports Medicine. 2023;51(7):1895-1903. doi:10.1177/03635465231171131
- Hamoodi Z, Winton J, Bhalaik V. Partial tear of the distal biceps tendon: Current concepts. J Orthop. 2022;32:18-24. doi:10.1016/j.jor.2022.05.002
- Allen J, Donoghue S, Rankin S, Andronic A, Archer J, Cowling P. Distal biceps injuries: an overview. Injury.Elsevier Ltd. 2025;56(8). doi:10.1016/j.injury.2025.112556
- Simpson ER, Jawanda H, Patel I, Verma NN, Parvaresh KC. No Clinically Significant Differences in Patient-Reported Outcomes and Range of Motion Between Early and Delayed Mobilization After Primary Distal Biceps Tendon Repair: A Systematic Review and Meta-analysis. American Journal of Sports Medicine. Published online November 1, 2025. doi:10.1177/03635465251317207
- Badon JT, Foster BK, Chen JS, et al. Preventing posterior interosseous nerve injury during a distal biceps tendon repair: an anatomic study comparing extensor digitorum communis and extensor carpi ulnaris muscle splitting approaches. J Shoulder Elbow Surg. Published online 2025. doi:10.1016/j.jse.2025.05.041
- MacLean SBM, Caekebeke P, Phadnis J, van Riet R, Bain GI. Current concepts in the aetiology, assessment and management of partial distal biceps tendon tears. Shoulder Elbow.SAGE Publications Inc. Preprint posted online 2024. doi:10.1177/17585732241245054
- Hogea B, Patrascu JM, Abu-Awwad SA, et al. Comparative Analysis of Surgical Approaches for Distal Biceps Tendon Rupture: Single-Incision Technique versus Double-Incision Technique. J Clin Med. 2023;12(19). doi:10.3390/jcm12196423
- Carrazana-Suarez LF, Cooke S, Schmidt CC. Return to Play After Distal Biceps Tendon Repair. doi:10.1007/s12178-022-09742-x/Published




