What is the meniscus?
The menisci are two fibrocartilaginous structures that are located between the femur and tibia. The menisci are C-shaped and are attached to the bone in the front and back of the tibia at root attachments. The periphery of the meniscus is attached to the tibia with coronary ligaments. The meniscus is composed of water, collagen and proteoglycans. The arrangement of the collagen and proteoglycans as well as bone attachments give the menisci their biomechanical properties.
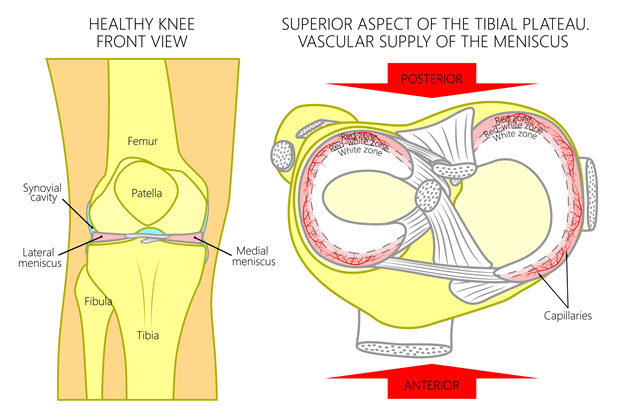 Figure 1 This figure shows both the normal medial and lateral menisci as well as blood supply.
Figure 1 This figure shows both the normal medial and lateral menisci as well as blood supply.
The menisci serve to aid in load transmission, shock absorption, stabilization and lubrication of the knee.
As the shape of the femur and tibia differ at the joint, the meniscus serves to fill the gap between the two bones and aid in load transmission.
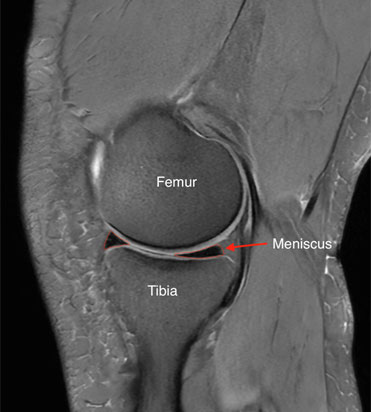 Figure 2 MRI of the knee demonstrating how the meniscus conforms to the shape of the femur and tibia. The meniscus is outlined in red.
Figure 2 MRI of the knee demonstrating how the meniscus conforms to the shape of the femur and tibia. The meniscus is outlined in red.
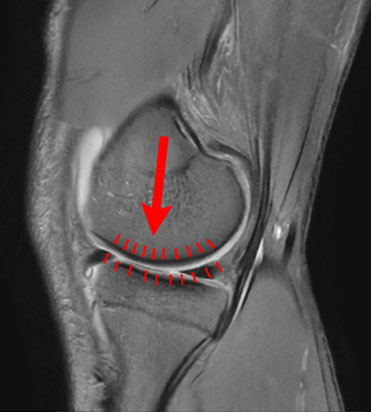 Figure 3 Arrows represent how load is spread throughout the knee along the meniscus.
Figure 3 Arrows represent how load is spread throughout the knee along the meniscus.
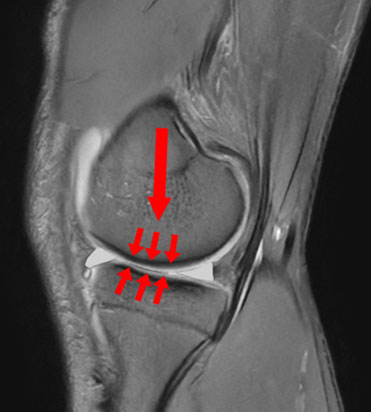 Figure 4 With the meniscus removed, larger arrows now represent increased load seen by the tibia.
Figure 4 With the meniscus removed, larger arrows now represent increased load seen by the tibia.
Shock absorption while walking occurs as the water portion of the meniscus is forced through the meniscus interstitial matrix giving the meniscus viscoelastic properties.
The shape and attachments of the menisci aid in providing additional stability to the knee. Both menisci move with knee flexion and extension. As the medial meniscus has more attachments, it serves a greater function in stability, acting as a secondary stabilizer in knees with an ACL tear.
The menisci function in lubrication of the knee by aiding in circulating knee synovial fluid during compression of the meniscus. Additionally, the presence of proteoglycans on the meniscus lower the amount of friction experienced by the knee.
What are the symptoms of a meniscus tear?
Symptoms of a meniscus tear will depend on the location of the tear, tear pattern and other factors. However, common symptoms include knee pain and swelling. Other symptoms may include catching, locking or giving out of the knee. Some large meniscus tears may even prevent full motion of the knee.
Are meniscus tears common?
Yes. Some estimate rates of 60-70 per 100,000 population. There is also an estimated 1 million meniscus surgeries performed in the US every year.
What causes meniscus tears?
Traumatic tears can occur from an increased load to the knee in either compression, rotation or shearing. This is common in sporting activities such as soccer, basketball, football and Jiu-Jitsu.
Degenerative tears occur as the meniscus loses elasticity and are associated with knee arthritis.
What are the types of meniscus tears?
Meniscus tears can be characterized as either traumatic or degenerative. There are also many different tear patterns of tears. Some examples of tear patterns include radial, horizontal, vertical, root, bucket handle and complex. Degenerative tears are often complex in appearance and are associated with arthritis. Meniscus root tears are located where the meniscus is attached to the tibia and often occur at the medial meniscus posterior root. Radial, bucket handle, horizontal and root tears, are associated with greater contact pressures in the knee.
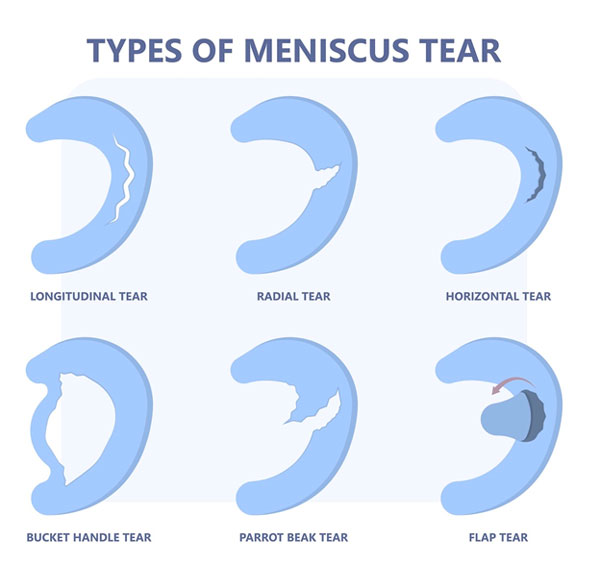 Figure 5 Views of meniscus tear types.
Figure 5 Views of meniscus tear types.
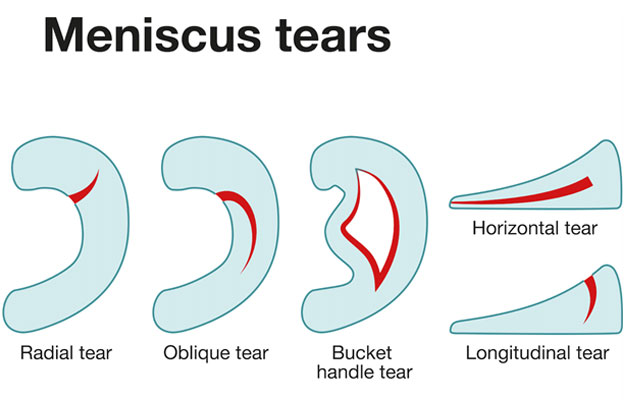 Figure 6 Additional views of meniscus tears.
Figure 6 Additional views of meniscus tears.
How are meniscus tears diagnosed?
Diagnosis begins with a history and physical examination. Examination may show tenderness at the knee where the meniscus is located. Special tests that apply stress to the meniscus may also be positive and suggest a tear. X-rays are also taken to evaluate for evidence of arthritis or other injuries to the bone. If a meniscus tear is suspected based on this an MRI is likely to be ordered to confirm the diagnosis.
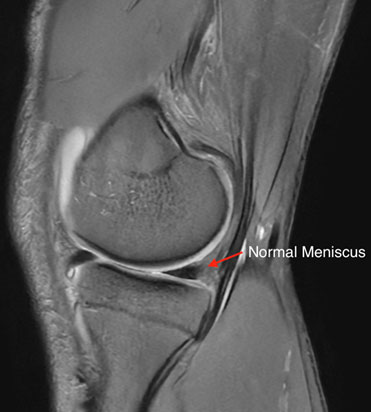 Figure 7 MRI example showing a normal appearing meniscus.
Figure 7 MRI example showing a normal appearing meniscus.
 Figure 8 MRI image of a medial meniscus tear with arrow pointing to the tear.
Figure 8 MRI image of a medial meniscus tear with arrow pointing to the tear.
How are meniscus tears treated?
Treatment for meniscus tears is individualized and based on many factors. Factors that are considered include, but are not limited to, mechanism of tear (traumatic or degenerative), pattern of the tear, location of the tear, symptoms, age of the patient, and activity level of the patient.
Nonoperative Treatment
Nonoperative treatment is often indicated for complex, degenerative meniscus tears. This can include anti-inflammatory medications and physical therapy. Injections such as platelet rich plasma have also been shown to be effective in pain relief.
Surgical Treatment
Surgical options include meniscectomy and meniscus repair.
A meniscectomy is a removal of the torn area of the meniscus. This is often colloquially referred to as a “clean up.” This can be indicated in certain degenerative meniscus tears that have failed nonoperative treatment. The procedure is performed with an arthroscope utilizing two small incisions. One incision is used to place a camera for visualization of the knee while the other is used to place the instruments used to resect the torn meniscus tissue.
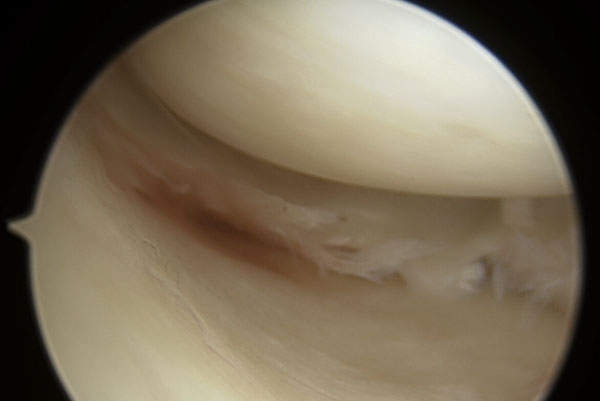 Figure 9 Arthroscopic view of a complex meniscus tear.
Figure 9 Arthroscopic view of a complex meniscus tear.
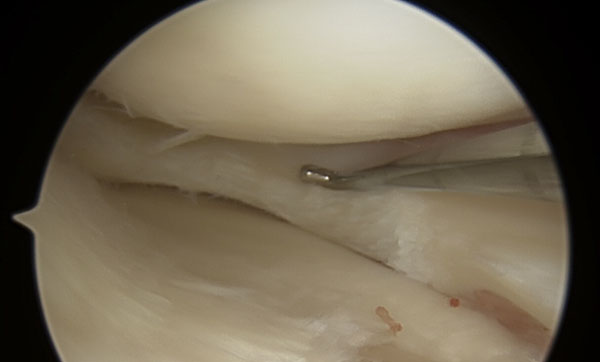 Figure 10 A view of the meniscus after a partial meniscectomy. An arthroscopic probe is seen in this view.
Figure 10 A view of the meniscus after a partial meniscectomy. An arthroscopic probe is seen in this view.
A meniscus repair involves placing sutures in or through the meniscus to allow the meniscus to heal. This is performed using the arthroscope as well. Many tear patterns can be repaired using two small incisions alone. However, certain other tear patterns may require the use of additional incisions. In the case of root tears, a drill tunnel in the tibia is often required to complete the repair.
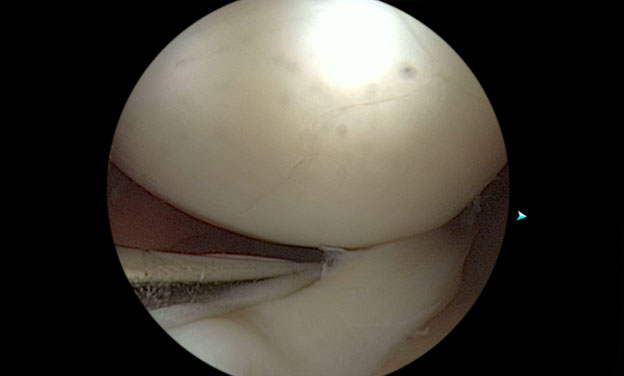 Figure 11 Large bucket handle meniscus tear. Probe in place shows displacement of the tear.
Figure 11 Large bucket handle meniscus tear. Probe in place shows displacement of the tear.
 Figure 12 After repair of the meniscus using an all inside type repair device.
Figure 12 After repair of the meniscus using an all inside type repair device.
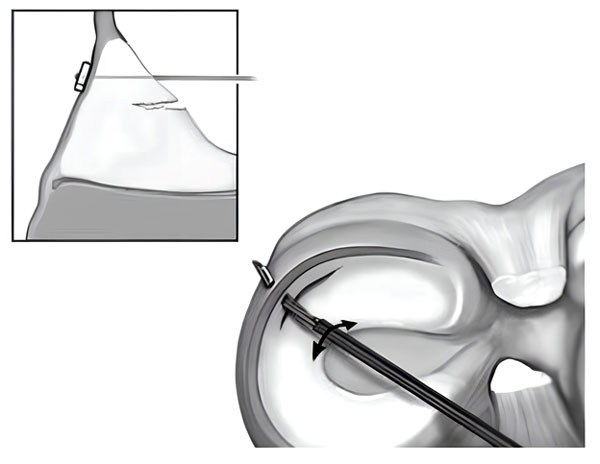 Figure 13 Illustration of all inside meniscus repair technique.
Figure 13 Illustration of all inside meniscus repair technique.
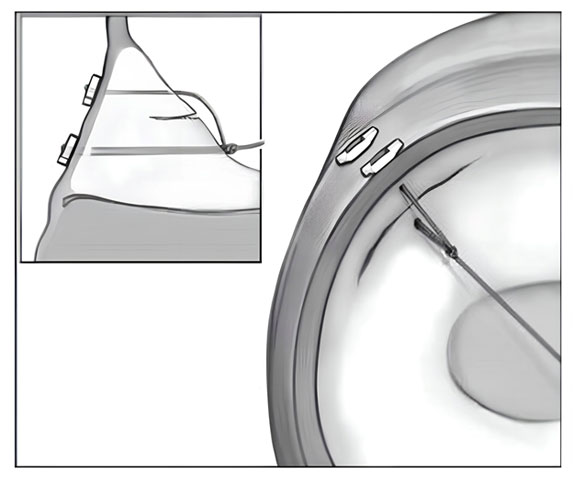 Figure 14 Illustration of all inside meniscus repair technique.
Figure 14 Illustration of all inside meniscus repair technique.
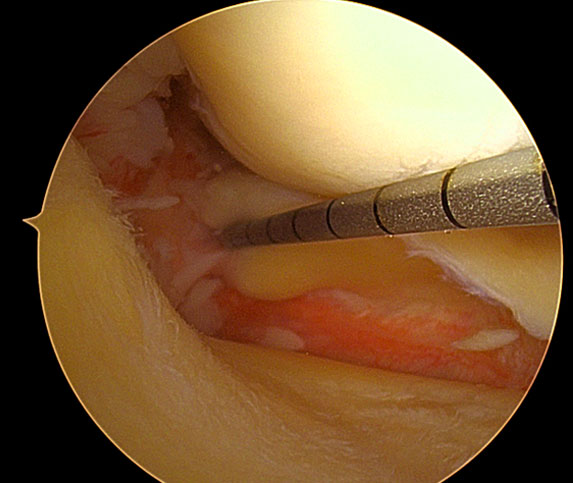 Figure 15 Meniscus root tear.
Figure 15 Meniscus root tear.
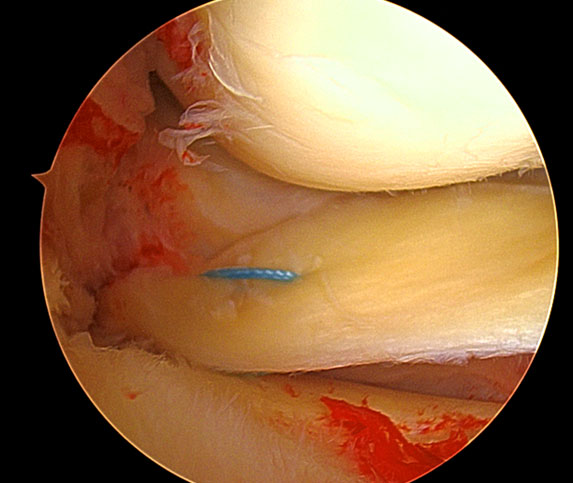 Figure 16 Example of root repair.
Figure 16 Example of root repair.
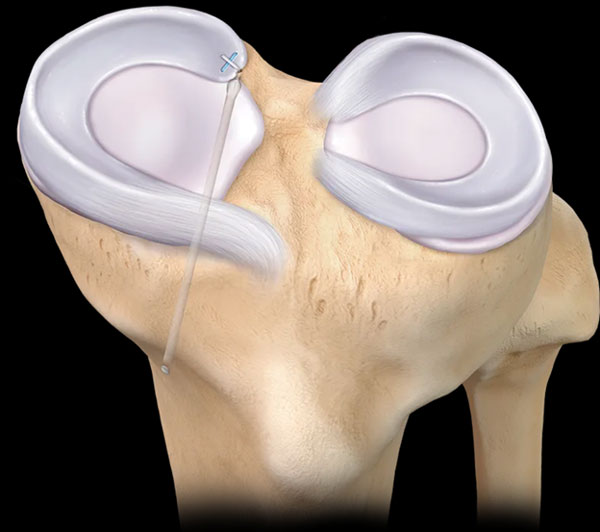 Figure 17 Illustration of a meniscus root repair. This technique involves drilling a tunnel in the tibia to repair the meniscus. Credit: Arthrex.com
Figure 17 Illustration of a meniscus root repair. This technique involves drilling a tunnel in the tibia to repair the meniscus. Credit: Arthrex.com
For certain patients, typically those that have previously had most of their meniscus removed, a meniscus transplant can also be performed. This uses an allograft meniscus from a donor to replace the meniscus tissue. This also uses tunnels and sutures to place the meniscus transplant.
Timing of Meniscus Surgery
For patients that have meniscus tears that are indicated for surgery, performing surgery sooner has shown to improve outcomes including healing after surgery.
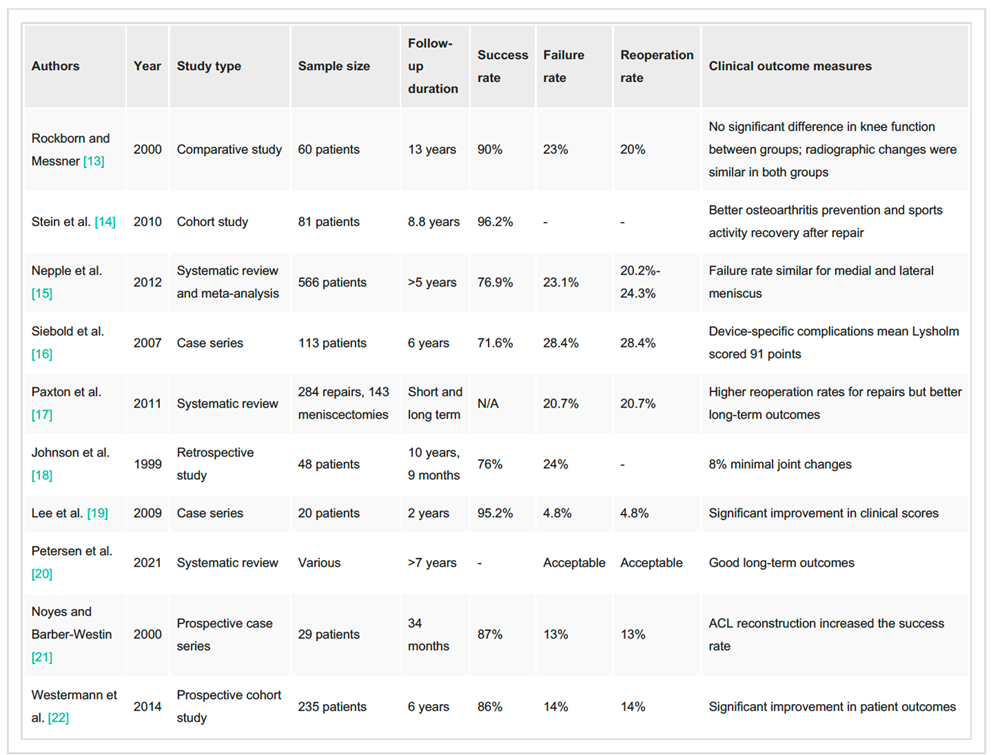
Outcomes of Meniscus Surgery
Outcomes of meniscus repair are generally favorable. Some reviews show success rates of ~83%. Certain tear types such as radial tears and meniscus root tears may have a lower healing rate.
Return to sport after meniscus surgery
Return to sport is based on many factors after a meniscus surgery. Factors that determine timing to return to sport include type of surgery performed (meniscectomy, repair or transplant), tear pattern, tissue quality, health and activity level of the patient, physical and psychological readiness. After meniscectomy the return to sport for many is 4-12 weeks after surgery. After meniscus repair the return to sport is often 4-9 months.
Complications after meniscus surgery
The following list includes the more common complications and is not exhaustive.
Infection
An uncommon complication reported rate of ~ 0.2%. Prevention at the time of surgery includes the surgical sterilization of the skin and using the use of antibiotics at the time of surgery. Presentation of infections could include fever, chills, increased pain and swelling at the surgical site, redness, warmth and drainage. Management often includes antibiotics and possibly surgical irrigation and debridement.
Repair Failure
Incidence of meniscus repair failure is roughly 20% depending on the series reported. Prevention includes appropriate surgical technique, rehabilitation, recovery and timing to return to activity. Treatment of repair failure may include revision repair or meniscectomy. Augmentation to aid in healing of the repair may include platelet rich plasma or bone marrow venting procedures.
Knee Stiffness
Knee stiffness results from scar tissue formation leading to restricted range of motion and rarely occurs after isolated meniscus repair. Prevention includes timing to surgery and accelerated rehabilitation protocols. Treatment of knee stiffness includes rehabilitation, surgical lysis of adhesions and manipulation under anesthesia.
Deep Venous Thrombosis (Blood clot)
Deep venous thrombosis is typically rare with reports being lower than 1% of cases. Presentation of a blood clot can include increased pain and swelling in the leg with diagnosis confirmed with an ultrasound. Prevention includes early immobilization, possible use of compression stockings, and possible use of chemical prophylaxis such as aspirin. Treatment typically includes use of anticoagulation medications such as lovenox or apixaban.
Nerve injury
Nerve injury is uncommon after meniscus surgery. Most common type of nerve injury includes numbness around incision sites. However, there are also reports of injury to the saphenous or peroneal nerves around the knee. This usually resolves with continued observation. In rare case pain management may be required to aid in symptom management.
Hardware Irritation
Hardware is used to repair the meniscus. Uncommonly this hardware can cause continued pain in the area it is located. This can present as localized pain and swelling at the hardware sites. In rare cases the hardware may need to be surgically removed once the repair has fully healed.
Osteoarthritis
Osteoarthritis development after a meniscus injury is multifactorial and ultimately related to cartilage injury and increased contact pressure. Progression may be more rapid in certain cases of meniscectomy or conservative care of meniscus tears. Prevention includes rehabilitation focusing on quadriceps strengthening and resorting joint mechanics and stability. Treatment may include anti inflammatory medications, injection therapy, rehabilitation and possible joint preservation surgery.
What will help my pain after surgery?
Medications including narcotic pain medications and anti inflammatories may be prescribed after surgery to help reduce pain. Nerve blocks at the time of surgery have been shown to be affective at reducing pain with low risk of long-term deficits. Additionally, use of cold compression devices has been shown to reduce pain and need for pain medications.
Are there other modalities that can improve my healing after meniscus surgery?
There are studies that show use of biologics such as platelet rich plasma can decrease of knee arthrofibrosis and improve healing of a meniscus repair. This can be injected at the time of surgery or after.
Neuromuscular Electrical Stimulation is used during knee rehabilitation to aid in muscle fiber recruitment. This can be applied both at home and during physical therapy sessions.
Use of blood flow restriction therapy involves use of a tourniquet like cuff placed on the lower extremity during exercise. Use of blood flow restriction therapy with low intensity exercise allows lower knee joint pain in comparison to high intensity training without blood flow restriction. This will be used during physical therapy sessions. Check with your physical therapy location if they have this modality available.
Supplement recommendations are often sought after surgery. There is low evidence to support the use of protein or collagen supplementation after surgery. No evidence is available to provide recommendations for a particular supplement. No significant evidence is available to support creatine supplementation or vitamin supplementation.
Do I need to use a brace after meniscus surgery?
In the immediate post operative period you will use a knee brace. The use of a knee brace that can lock in extension can prevent knee buckling while walking in the immediate post operative period. It is also used to prevent excessive knee flexion that may put excessive strain on the meniscus repair.
The use of knee bracing when return to sport is controversial. Functional knee bracing has been shown to have benefits in proprioception and limb symmetry. However, clinical studies show no significant benefit in functional stability, patient reported outcomes or retear rates. Your use of a brace will largely be determined on subjective stability, sporting type and activity level.
When can I return to work after surgery?
Return to work will largely depend on your specific occupational requirements. Many patients are no longer requiring the use of pain medications during the day by the fifth day after surgery. If your work is sedentary, you may be able to return as soon as this time. If you are required to stand for a significant period during the day return to work may need to be delayed until you are off crutches. This may be from week 1-6 after surgery depending on whether a meniscectomy or repair was performed. Work that involves heavy lifting may require longer periods away from work if light duty is not available.
When can I drive after surgery?
There is no definitive test we can do to determine when a patient is safe to return to driving. You should not be taking narcotic or sedating medications prior to driving. Studies attempting to look at when it is safe to return to driving have looked at brake response times. There are no definitive studies looking at isolated meniscus repair but in general guidelines following ACL reconstruction can be followed. In general, brake response time has been shown to return to normal by 4-6 weeks after right sided ACL surgery and 2-3 weeks after left sided ACL surgery.
Post operative Instructions
- Following your stay in the recovery room and when your vital signs are stable you will be discharged to your escort.
- Remember, it is normal to feel a little dizzy or drowsy for several hours after surgery. This is due to the action the medicine used during surgery.
- If you do not have a post operative appointment scheduled, please call the office as soon as possible to schedule this appointment.
- Take your pain medicine as directed. Begin the pain medicine before you start getting uncomfortable, as the nerve block will wear off. If you wait to take your pain medication until the pain is severe, you will have more difficulty in controlling the pain.
- Take 1 tablet (81 mg) of aspirin per day, starting the day after surgery and continuing for 4 weeks. The risk of blood clots is quite low after meniscus surgery, but aspirin is taken as a precaution to decrease the risk. Certain factors such as smoking, birth control pills and certain medical conditions increase the risk of blood clots, and it is especially important to take the aspirin for those situations. If you were previously on a blood thinner you will resume this medication, rather than starting aspirin, beginning the day after surgery.
- If you are taking narcotic pain medication you may need a stool softener to prevent constipation. Over-the-counter medication such as Docusate or Milk of Magnesia is recommended.
- Notify the office of any fever, chills, or temperature > 100.5.
- Notify the office of any wound drainage.
- You can begin the home exercises listed below the day after surgery. Perform the ankle pumps periodically, throughout the day. The remainder of the exercises can be performed once at least once a day.
Post-Surgery Diet
Resume your diet as tolerated and include vegetables, fruits, and proteins (such as meats, fish, chicken, nuts, and eggs) to promote healing. Also, remember to have adequate fluid intake. It is common after surgery to lack an appetite. This may be the result of anesthesia and the medications. Proper nutrition is needed for healing. During the healing process, the body needs increased amounts of calories and protein. Eat a variety of foods to get all the calories, proteins, vitamins, and minerals you need. If you have been told to follow a specific diet, please follow it.
If you’re not eating well after surgery, contact your healthcare provider about nutritional supplements.
How should I manage my surgical site and bandages?
You can remove your surgical dressing on the third day after your surgery. You will remove everything except the Steri-strips if present. See picture below for example of Steri strips.
Allow the steri-strips to fall off on their own. If necessary, sutures will be removed at your first post-operative visit.
Example of Steri strips:

You may shower with a waterproof bandage covering the incisions in three days. Example of waterproof bandage shown in picture below. These can typically be purchased at CVS or Walgreens. Keep the incisions dry until the Steri strips fall off or are removed in clinic. Try not to let the direct spray of water from the showerhead hit the incision.
You can cover your incision with a bandage if needed to prevent irritation with clothing.
A small amount of drainage from the surgical sites is common. If this occurs, you may apply a bandage to the affected area.
Leakage immediately after surgery is normal and helps to drain some of the fluid that accumulates in the joint during surgery.
The dressings may become moist or blood-stained; this is normal and not typically a cause for alarm.
Example of waterproof bandage:

Do I need to wear a knee brace?
You will use a knee brace such as this:

Instructions for fitting and adjustment can be found at:
https://www.breg.com/products/knee-bracing/post-op/t-scope-premier-post-op-knee-brace/
You will lock the brace straight when walking but can unlock the brace at rest. The prescribed range of motion settings will be set in the operating room.
You may remove the knee brace for exercises as prescribed by the surgeon/therapist, icing, dressing, and showering.
What is my activity level after surgery?
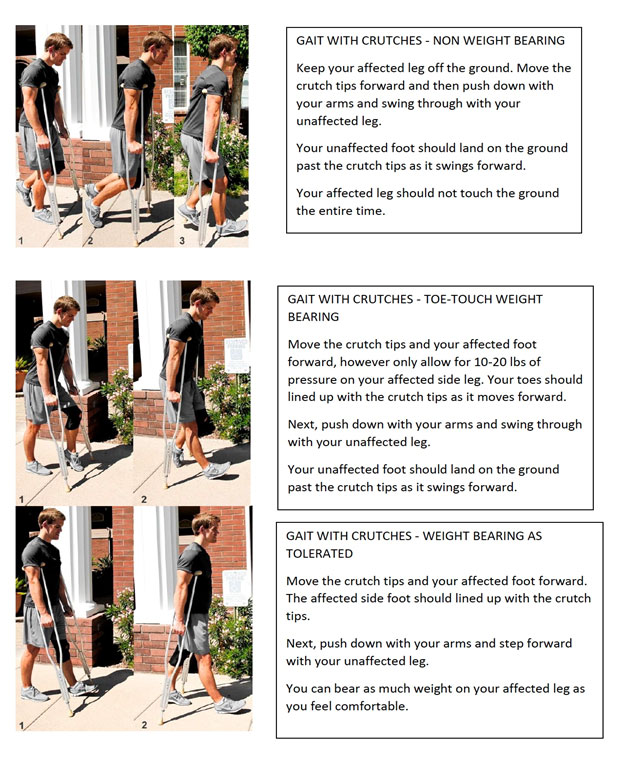
You will use crutches to aid with walking after surgery.
Elevate the operative leg to chest level whenever possible to decrease swelling. Do not place pillows under knees (i.e. do not maintain knee in a flexed or bent position) but rather place pillows under foot/ankle.
Do not engage in activities which increase knee pain/swelling (prolonged periods of standing or walking) over the first 7-10 days following surgery.
Avoid long periods of sitting (without leg elevated) or long distance traveling for 2 weeks.
Physical therapy should begin by post-operative day 5 or sooner.
You can begin motion of your ankle and toes now.
How do I use my ice machine?
Use of cold compression can help with post operative pain and swelling after surgery. One example is the following:

Instructions for use can be found at:
https://www.breg.com/products/cold-therapy/devices/polar-care-wave/
If you have another machine please check that manufacturer’s website for use instructions.
Use every waking hour for 15 minutes for the first 24 hours. After this time you can use the machine at least three times a day for 15 minutes.
Do not sleep with the automated device on.
Keep a layer of fabric between the skin and icing device at all times.
How do I use the neuromuscular electrical stimulation?
An example of an NMES machine includes:
Instructions for use can be found at:
https://www.zynex.com/products/nexwave/
Electrodes will be placed at the quadriceps. For example:
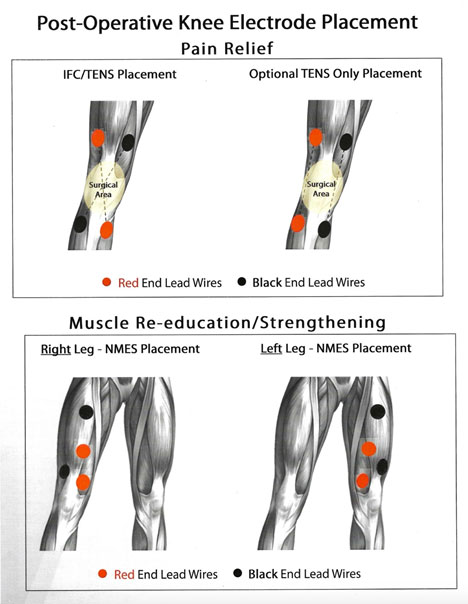
With the knee in extension, increase the stimulation amplitude until contraction of the quadriceps is visualized. Increase amplitude to your tolerance level. Contractions should last 10 seconds with 30-50 second rest periods between contractions. This can be started once the bandages are removed on the third day after surgery. This can be performed at least 5 days a week for one hour per day.
Can I smoke following surgery?
You should not smoke after surgery as it interferes with healing.
Questions or Concerns
If at any time you have questions or concerns you can either contact your surgeon’s medical assistant via email or you can call the main office numbers at: 855-624-3306. You can also use the electronic medical record’s online portal to send questions.
Exercises you can perform at home at this time:
 Straight Leg Raise
Straight Leg Raise
While lying on your back, raise up your leg with a straight knee. Keep the opposite knee bent with the foot planted on the ground.
 Short Arc Quad
Short Arc Quad
Place a rolled up towel or object under your knee and slowly straighten your knee as you raise up your foot.
 Heel Slides- Supine
Heel Slides- Supine
Lying on your back with knees straight, slide the affected heel towards your buttocks as you bend your knee. Hold a gentle stretch in this position and then return to original position.
 Ankle Pumps
Ankle Pumps
Bend your foot up and down at your ankle joint as shown.
- Kamaci S, Pace JL. Redefining Failure: Criteria for Unsuccessful Outcomes in Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(9):353-360. doi:10.1007/s12178-025-09971-w
- Villarreal-Espinosa JB, Berreta RS, Pallone L, et al. Failure and complication rates following meniscal all-inside and inside-out repairs: A systematic review and meta-analysis. Knee Surgery, Sports Traumatology, Arthroscopy. 2025;33(6):1992-2009. doi:10.1002/ksa.12485
- van der List JP, Daniel S, Blom I, Benner JL. Early Meniscal Repair Leads to Higher Success Rates Than Delayed Meniscal Repair: A Systematic Review and Meta-analysis. American Journal of Sports Medicine. Published online September 1, 2025. doi:10.1177/03635465241298619
- Quesnot A, Mouchel S, Salah S Ben, Baranes I, Martinez L, Billuart F. Randomized controlled trial of compressive cryotherapy versus standard cryotherapy after total knee arthroplasty: pain, swelling, range of motion and functional recovery. BMC Musculoskelet Disord. 2024;25(1). doi:10.1186/s12891-024-07310-7
- Cabarcas B, Peairs E, Iyer S, et al. Long-Term Results for Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(7):229-245. doi:10.1007/s12178-025-09966-7
- Szőcs GF, Váncsa S, Agócs G, et al. Does concomitant meniscus repair and meniscectomy show different efficacy in anterior cruciate ligament reconstruction? A systematic review and meta-analysis. J Orthop Translat.Elsevier (Singapore) Pte Ltd. 2024;48:1-10. doi:10.1016/j.jot.2024.07.004
- Orellana F, Grassi A, Hlushchuk R, et al. Revealing the complexity of meniscus microvasculature through 3D visualization and analysis. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-61497-2
- Chand SB, Santhosh G, Saseendran A, et al. Efficacy and Long-Term Outcomes of Arthroscopic Meniscus Repair: A Systematic Review and Meta-Analysis. Cureus. Published online October 4, 2024. doi:10.7759/cureus.70828
- Lee DR, Lu Y, Reinholz AK, et al. Root Repair Has Superior Radiological and Clinical Outcomes Than Partial Meniscectomy and Nonoperative Treatment in the Management of Meniscus Root Tears: A Systematic Review. Arthroscopy - Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2025;41(2):390-417. doi:10.1016/j.arthro.2024.02.017
- Kuczyński N, Boś J, Białoskórska K, et al. The Meniscus: Basic Science and Therapeutic Approaches. J Clin Med.Multidisciplinary Digital Publishing Institute (MDPI). 2025;14(6). doi:10.3390/jcm14062020
- Li Z, Weng X. Platelet-rich plasma use in meniscus repair treatment: a systematic review and meta-analysis of clinical studies. J Orthop Surg Res.BioMed Central Ltd. 2022;17(1). doi:10.1186/s13018-022-03293-0
- Lee DR, Lu Y, Reinholz AK, et al. Root Repair Has Superior Radiological and Clinical Outcomes Than Partial Meniscectomy and Nonoperative Treatment in the Management of Meniscus Root Tears: A Systematic Review. Arthroscopy - Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2025;41(2):390-417. doi:10.1016/j.arthro.2024.02.017
- Golz AG, Mandelbaum & B, Pace JL. All-Inside Meniscus Repair. doi:10.1007/s12178-022-09766-3/Published
- Cabarcas B, Peairs E, Iyer S, et al. Long-Term Results for Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(7):229-245. doi:10.1007/s12178-025-09966-7
- Peng Y, Lu M, Zhou Z, et al. Natural biopolymer scaffold for meniscus tissue engineering. Front Bioeng Biotechnol.Frontiers Media S.A. 2022;10. doi:10.3389/fbioe.2022.1003484
- Ozeki N, Seil R, Krych AJ, Koga H. Surgical treatment of complex meniscus tear and disease: State of the art. Journal of ISAKOS.BMJ Publishing Group. 2021;6(1):35-45. doi:10.1136/jisakos-2019-000380
- Śmigielski R, Azua E, Gursoy S, et al. A Novel Description of Medial Meniscus Vascularization: A Multicenter Study Introducing the “Medial Meniscal Artery.” American Journal of Sports Medicine. 2024;52(14):3551-3560. doi:10.1177/03635465241291802
- Tschopp B, Omoumi P, Nyland J, et al. Knee malalignment and laterality influence 2-year meniscus tear repair outcomes: A pilot study. Knee Surgery, Sports Traumatology, Arthroscopy. Published online October 1, 2025. doi:10.1002/ksa.12602
- Chand SB, Santhosh G, Saseendran A, et al. Efficacy and Long-Term Outcomes of Arthroscopic Meniscus Repair: A Systematic Review and Meta-Analysis. Cureus. Published online October 4, 2024. doi:10.7759/cureus.70828
- Posadzy M, Joseph GB, McCulloch CE, et al. Natural history of new horizontal meniscal tears in individuals at risk for and with mild to moderate osteoarthritis: data from osteoarthritis initiative. Eur Radiol. 2020;30(11):5971-5980. doi:10.1007/s00330-020-06960-0
- Gross PW, Jones RH, Beber SA, Farrell AM, Fabricant PD. Assessing the Risk of Injury to the Popliteal Neurovascular Bundle during Lateral Meniscus Repair: A Case Report. J Orthop Case Rep. 2025;15(5):61-64. doi:10.13107/jocr.2025.v15.i05.5556
- Karjalainen VP, Kestilä I, Finnilä MA, et al. Quantitative three-dimensional collagen orientation analysis of human meniscus posterior horn in health and osteoarthritis using micro-computed tomography. Osteoarthritis Cartilage. 2021;29(5):762-772. doi:10.1016/j.joca.2021.01.009
- Floyd ER, Rodriguez AN, Falaas KL, et al. The Natural History of Medial Meniscal Root Tears: A Biomechanical and Clinical Case Perspective. Front Bioeng Biotechnol. 2021;9. doi:10.3389/fbioe.2021.744065
- Lee DI, Lovejoy RJ, Jones MH, Matzkin EG, Katz JN. The evolution of the meniscus: Where surgical advancements meet translational research. Osteoarthr Cartil Open. 2025;7(4). doi:10.1016/j.ocarto.2025.100666
- Farinelli L, Meena A, Montini D, et al. Failure rate of isolated medial meniscus repair in the stable knee: Systematic review and meta-analysis. Knee Surgery, Sports Traumatology, Arthroscopy. 2025;33(4):1333-1344. doi:10.1002/ksa.12441
- Guo H, Li Q, Zhang Z, et al. Better clinical outcomes and return to sport rates with additional medial meniscus root tear repair in high tibial osteotomy for medial compartmental knee osteoarthritis. Knee Surgery, Sports Traumatology, Arthroscopy. 2024;32(7):1753-1765. doi:10.1002/ksa.12180
- Bhatia S, Laprade CM, Ellman MB, Laprade RF. Meniscal root tears: Significance, diagnosis, and treatment. American Journal of Sports Medicine. 2014;42(12):3016-3030. doi:10.1177/0363546514524162
- Shiwaku K, Otsubo H, Takahashi K, et al. Biomechanical Comparison of Inside-Out and All-Inside Meniscal Repair in Controlling the Peripheral Gap and Extrusion of the Lateral Meniscus With a Complete Radial Tear: A Cadaveric Study Using a Robotic Simulator. Orthop J Sports Med. 2025;13(3). doi:10.1177/23259671241308854
- Monson JK, Tollefson L V., LaPrade CM, LaPrade RF. Current Rehabilitation Principles Following Meniscus Repairs. Curr Rev Musculoskelet Med.Springer. 2025;18(9):331-343. doi:10.1007/s12178-025-09967-6
- Sedgwick MJ, Saunders C, Getgood AMJ. Systematic Review and Meta-analysis of Clinical Outcomes Following Meniscus Repair in Patients 40 Years and Older. Orthop J Sports Med. 2024;12(8). doi:10.1177/23259671241258974
- Fox AJS, Bedi A, Rodeo SA. The Basic Science of Human Knee Menisci: Structure, Composition, and Function. Sports Health. 2012;4(4):340-351. doi:10.1177/1941738111429419
- Chen KH, Ma HH, Fu A, Wang HY, Ma HL, Chiang ER. Arthroscopic all-inside wrapping repair of lateral meniscus bucket-handle tears: clinical and imaging outcomes. J Orthop Surg Res. 2025;20(1). doi:10.1186/s13018-025-05489-6
- Dzidzishvili L, Berreta RS, Jackson GR, et al. All-Inside and Inside-Out Repair Techniques for Bucket-Handle Meniscus Tears Both Result in Improved Patient Outcomes and a Broad Range of Failure Rates: A Systematic Review. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2024;40(9):2477-2490.e1. doi:10.1016/j.arthro.2024.01.021
- Deichsel A, Peez C, Raschke MJ, et al. Arthroscopic Centralization of the Medial Meniscus Reduces Load on a Posterior Root Repair Under Dynamic Varus Loading: A Biomechanical Investigation. American Journal of Sports Medicine. 2024;52(12):3030-3038. doi:10.1177/03635465241274791
- Utrilla GS, Degano IR, D’Ambrosi R. Efficacy of platelet-rich plasma in meniscal repair surgery: a systematic review of randomized controlled trials. Journal of Orthopaedics and Traumatology.Springer Science and Business Media Deutschland GmbH. 2024;25(1). doi:10.1186/s10195-024-00799-7
- Choi BS, Won J, Han HS. Augmentation with Bone Marrow Aspirate Harvested from the Iliac Crest for Horizontal or Radial Meniscal Tears Yields Favorable Healing Rates in Magnetic Resonance Imaging and Clinical Outcomes. CiOS Clinics in Orthopedic Surgery. 2024;16(6):897-905. doi:10.4055/cios23213
- Barber FA, Howard MS, Ashraf W, Spenciner DB. The Biomechanical Performance of the Latest All-Inside Meniscal Repair Devices. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2020;36(12):3001-3007. doi:10.1016/j.arthro.2020.03.036
- Monson JK, Tollefson L V., LaPrade CM, LaPrade RF. Current Rehabilitation Principles Following Meniscus Repairs. Curr Rev Musculoskelet Med.Springer. 2025;18(9):331-343. doi:10.1007/s12178-025-09967-6
- Chen K, Aggarwal S, Baker H, Athiviraham A. Biologic Augmentation of Isolated Meniscal Repair. Current Reviews in Musculoskeletal Medicine .Springer. 2024;17(7):223-234. doi:10.1007/s12178-024-09898-8
- Tollefson L V., Tuca MJ, Tapasvi S, LaPrade RF. Medial meniscus ramp tears: State of the art. Journal of ISAKOS.Elsevier Inc. 2025;10. doi:10.1016/j.jisako.2024.100380
- Kamaci S, Pace JL. Redefining Failure: Criteria for Unsuccessful Outcomes in Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(9):353-360. doi:10.1007/s12178-025-09971-w
- Ishibashi Y, Sasaki E, Kimura Y, Tsushima T. Delta-Grip Stitch for Medial Meniscus Posterior Root Repair. Arthrosc Tech. 2024;13(7). doi:10.1016/j.eats.2024.102999
- Kamaci S, Pace JL. Redefining Failure: Criteria for Unsuccessful Outcomes in Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(9):353-360. doi:10.1007/s12178-025-09971-w
- Jildeh TR, Okoroha KR, Kuhlmann N, Cross A, Abbas MJ, Moutzouros V. Multimodal Nonopioid Pain Protocol Provides Equivalent Pain Versus Opioid Control Following Meniscus Surgery: A Prospective Randomized Controlled Trial. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2021;37(7):2237-2245. doi:10.1016/j.arthro.2021.02.043
- Feroe AG, Clark SC, Hevesi M, et al. Management of Meniscus Pathology with Concomitant Anterior Cruciate Ligament Injury. Current Reviews in Musculoskeletal Medicine .Springer. 2024;17(8):321-334. doi:10.1007/s12178-024-09906-x
- Moon HS, Choi CH, Jung M, et al. Association Between Insufficient Restoration of Meniscal Tension During Surgical Repair of Medial Meniscus Root Tear and Surgical Outcomes: Clinical Implication of Curtain-Cliff Sign. American Journal of Sports Medicine. 2025;53(1):163-171. doi:10.1177/03635465241293733
- Gerhold C, Dave U, Bi AS, Chahla J. Medial Meniscus Root Tears: Anatomy, Repair Options, and Outcomes. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2025;41(4):871-873. doi:10.1016/j.arthro.2025.01.005
- Vivekanantha P, Thomas R, Kaplan G, Ho M, de SA D, Kay J. Surgical Management of the Discoid Lateral Meniscus: a Systematic Review of Outcomes. Curr Rev Musculoskelet Med.Springer. Preprint posted online November 1, 2025. doi:10.1007/s12178-025-09980-9
- Mameri ES, Jackson GR, Gonzalez F, et al. Meniscus Radial Tears: Current Concepts on Management and Repair Techniques. Curr Rev Musculoskelet Med.Springer. 2023;16(5):182-191. doi:10.1007/s12178-023-09831-5
- Pujol N, Giordano AO, Wong SE, et al. The formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT initiative. Part I—Rehabilitation management after meniscus surgery (meniscectomy, repair and reconstruction). Knee Surgery, Sports Traumatology, Arthroscopy. 2025;33(8):3002-3013. doi:10.1002/ksa.12674
- Strony JT, Mengers S, Sivasundaram L, et al. An Opioid-Sparing Pain Protocol of Intravenous and Oral Ketorolac Reduces Opioid Consumption and Pain Levels After Arthroscopic Meniscus Surgery: A Prospective, Randomized Controlled Trial. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2025;41(6):1989-2001.e1. doi:10.1016/j.arthro.2024.08.035
- Castle JP, Tramer JS, Turner EHG, et al. Survey of blood flow restriction therapy for rehabilitation in Sports Medicine patients. J Orthop. 2023;38:47-52. doi:10.1016/j.jor.2023.03.007
- Vint H, Quartley M, Robinson JR. All-inside versus inside-out meniscal repair: A systematic review and meta-analysis. Knee. 2021;28:326-337. doi:10.1016/j.knee.2020.12.005
- Kamaci S, Pace JL. Redefining Failure: Criteria for Unsuccessful Outcomes in Meniscus Repair. Curr Rev Musculoskelet Med.Springer. 2025;18(9):353-360. doi:10.1007/s12178-025-09971-w
- Phillips AR, Haneberg EC, Boden SA, Yanke AB, Cole BJ. Long-Term Clinical and Radiographic Outcomes of Meniscus Allograft Transplant. Curr Rev Musculoskelet Med.Springer. 2024;17(9):343-352. doi:10.1007/s12178-024-09904-z
- Karam KM, Moussa MK, Noailles T, et al. Postoperative Cryotherapy in Joints Other Than the Knee: A Systematic Review of Pain, Edema, Analgesic Use, and Blood Loss in the Shoulder, Hand, Hip, and Ankle Joints. Orthop J Sports Med.SAGE Publications Ltd. 2025;13(3). doi:10.1177/23259671251320132
- Kunkle BF, Kothandaraman V, Goodloe JB, et al. Orthopaedic Application of Cryotherapy: A Comprehensive Review of the History, Basic Science, Methods, and Clinical Effectiveness. JBJS Rev.Journal of Bone and Joint Surgery Inc. 2021;9(1). doi:10.2106/JBJS.RVW.20.00016
- Vivekanantha P, Thomas R, Kaplan G, Ho M, de SA D, Kay J. Surgical Management of the Discoid Lateral Meniscus: a Systematic Review of Outcomes. Curr Rev Musculoskelet Med.Springer. Preprint posted online November 1, 2025. doi:10.1007/s12178-025-09980-9
- Lai WC, Mange TR, Karasavvidis T, Lee YP, Wang D. Low early complication rates after arthroscopic meniscus repair and meniscectomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2023;31(10):4117-4123. doi:10.1007/s00167-023-07507-8
- Berzolla E, Sundaram V, Strauss E. A Review of Revision Meniscal Repair: Clinical Considerations and Outcomes. Curr Rev Musculoskelet Med.Springer. 2025;18(9):344-352. doi:10.1007/s12178-025-09968-5
- Gerhold C, Dave U, Bi AS, Chahla J. Medial Meniscus Root Tears: Anatomy, Repair Options, and Outcomes. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2025;41(4):871-873. doi:10.1016/j.arthro.2025.01.005
- Benhenneda R, Alajji M, Portet A, Sonnery-Cottet B, Fayard JM, Thaunat M. Repair of radial tears of the lateral meniscus on a stable knee: Results at a minimum follow-up of 2 years. Orthopaedics and Traumatology: Surgery and Research . 2024;110(4). doi:10.1016/j.otsr.2024.103877
- Noorduyn JCA, Van De Graaf VA, Willigenburg NW, et al. Effect of Physical Therapy vs Arthroscopic Partial Meniscectomy in People with Degenerative Meniscal Tears: Five-Year Follow-up of the ESCAPE Randomized Clinical Trial. JAMA Netw Open. 2022;5(7):E2220394. doi:10.1001/jamanetworkopen.2022.20394
- Hutchinson ID, Moran CJ, Potter HG, Warren RF, Rodeo SA. Restoration of the meniscus: Form and function. American Journal of Sports Medicine. 2014;42(4):987-998. doi:10.1177/0363546513498503
- Gurba JE, Weiss-Laxer NS, Haider MN, Marzo JM. Patient-reported Outcomes After Medial Meniscus Root Tear Repair Versus Other Medial Meniscus Repairs: An Exploratory Meta-analysis of Single-arm Cohorts. J Am Acad Orthop Surg Glob Res Rev. 2024;8(9). doi:10.5435/JAAOSGlobal-D-23-00293
- Nin DZ, Chen YW, Mandalia K, et al. Costs and Timing of Surgery in the Management of Meniscal Tears. Orthop J Sports Med. 2024;12(7). doi:10.1177/23259671241257881
- Alhamdi H, Foissey C, Vieira TD, et al. High failure rate after medial meniscus bucket handle tears repair in the stable knee. Orthopaedics and Traumatology: Surgery and Research . 2024;110(4). doi:10.1016/j.otsr.2023.103737
- Berzolla E, Sundaram V, Strauss E. A Review of Revision Meniscal Repair: Clinical Considerations and Outcomes. Curr Rev Musculoskelet Med.Springer. 2025;18(9):344-352. doi:10.1007/s12178-025-09968-5
- Hohmann E. Treatment of Degenerative Meniscus Tears. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2023;39(4):911-912. doi:10.1016/j.arthro.2022.12.002
- Marigi EM, Davies MR, Marx RG, Rodeo SA, Williams RJ. Meniscus Tears in Elite Athletes: Treatment Considerations, Clinical Outcomes, and Return to Play. Current Reviews in Musculoskeletal Medicine .Springer. 2024;17(8):313-320. doi:10.1007/s12178-024-09907-w
- Perrotta C, Chahla J, Badariotti G, Ramos J. Interventions for preventing venous thromboembolism in adults undergoing knee arthroscopy. Cochrane Database of Systematic Reviews.John Wiley and Sons Ltd. 2022;2022(8). doi:10.1002/14651858.CD005259.pub5
- Mallory N, Qin C, Gibbs D, et al. Horizontal Cleavage Meniscus Tears: Biomechanics, Indications, Techniques, and Outcomes. JBJS Rev.Journal of Bone and Joint Surgery Inc. 2023;11(8). doi:10.2106/JBJS.RVW.23.00042
- Berg B, Roos EM, Englund M, et al. Arthroscopic partial meniscectomy versus exercise therapy for degenerative meniscal tears: 10-year follow-up of the OMEX randomised controlled trial. Br J Sports Med. 2025;59(2):91-98. doi:10.1136/bjsports-2024-108644
- Markes AR, Hodax JD, Ma CB. Meniscus Form and Function. Clin Sports Med.W.B. Saunders. 2020;39(1):1-12. doi:10.1016/j.csm.2019.08.007
- Nin DZ, Chen YW, Mandalia K, et al. Costs and Timing of Surgery in the Management of Meniscal Tears. Orthop J Sports Med. 2024;12(7). doi:10.1177/23259671241257881
- Ford BT, Kong R, Wellington IJ, et al. Impact of Obesity, Smoking, and Age on 30-Day Postoperative Outcomes of Patients Undergoing Arthroscopic Meniscus Surgery. Orthopedics. 2024;47(6):332-336. doi:10.3928/01477447-20240826-04
- Fox AJS, Wanivenhaus F, Burge AJ, Warren RF, Rodeo SA. The human meniscus: A review of anatomy, function, injury, and advances in treatment. Clinical Anatomy.John Wiley and Sons Inc. 2015;28(2):269-287. doi:10.1002/ca.22456
- de Vries AJ, Aksakal HK, Brouwer RW. Effects of 6 weeks of cryotherapy plus compression therapy after total or unicompartmental knee arthroplasty: protocol for a single-centre, single-blind randomised controlled trial. BMJ Open. 2024;14(1). doi:10.1136/bmjopen-2023-077614
- Elphingstone JW, Alston ET, Colorado BS. Platelet-rich plasma for nonoperative management of degenerative meniscal tears: A systematic review. J Orthop.Reed Elsevier India Pvt. Ltd. 2024;54:67-75. doi:10.1016/j.jor.2024.03.009
- Sheasley JA, Kirby JC, Niu EL, et al. Characteristics and Outcomes of Operatively Treated Discoid Lateral Meniscus in Pediatric and Young Adult Patients: A Multicenter Study. American Journal of Sports Medicine. 2024;52(11):2758-2763. doi:10.1177/03635465241272393
- Flores SE, Manatrakul R, Anigwe C, et al. Prognostic Factors on Preoperative MRI for Patient-Reported Outcomes After Posterior Medial Meniscus Root Repair. Orthop J Sports Med. 2024;12(8). doi:10.1177/23259671241263648
- Ahmed I, Radhakrishnan A, Khatri C, et al. Meniscal tears are more common than previously identified, however, less than a quarter of people with a tear undergo arthroscopy. Knee Surgery, Sports Traumatology, Arthroscopy. 2021;29(11):3892-3898. doi:10.1007/s00167-021-06458-2
- Wiley TJ, Lemme NJ, Marcaccio S, et al. Return to Play Following Meniscal Repair. Clin Sports Med.W.B. Saunders. 2020;39(1):185-196. doi:10.1016/j.csm.2019.08.002
- Gronbeck KR, Tompkins MA. Functional testing following isolated meniscus repair may help to identify patients who need additional physical therapy prior to a return to activity. Journal of ISAKOS. 2024;9(4):557-561. doi:10.1016/j.jisako.2024.04.007
- Gee SM, Posner M. Meniscus Anatomy and Basic Science. Vol 29.; 2021. www.sportsmedarthro.com
- Prill R, Ma CB, Wong SE, et al. The Formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT Initiative Part II—Prevention, Nonoperative Treatment and Return to Sport. Orthop J Sports Med. 2025;13(6). doi:10.1177/23259671251349553
- Massey PA, Scalisi W, Montgomery C, Daily D, Robinson J, Solitro GF. Biomechanical Comparison of All-Suture, All-Inside Meniscus Repair Devices in a Human Cadaveric Meniscus Model. Cartilage. 2025;16(2):150-158. doi:10.1177/19476035241234315
- Pujol N, Giordano AO, Wong SE, et al. The Formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT Initiative: Part I—Rehabilitation Management After Meniscus Surgery (Meniscectomy, Repair and Reconstruction). Orthop J Sports Med. 2025;13(5). doi:10.1177/23259671251343088
- Wiley TJ, Lemme NJ, Marcaccio S, et al. Return to Play Following Meniscal Repair. Clin Sports Med.W.B. Saunders. 2020;39(1):185-196. doi:10.1016/j.csm.2019.08.002




